
What is anterior crossbite? (Underbite)
`Anterior crossbite (underbite) is an abnormal labiolingual relationship between one or more maxillary and mandibular incisor teeth (1). It can be functional and skeletal. `

What causes anterior crossbite? (Etiology)
Common causes of anterior crossbite are dental or skeletal origins.
1. Dental problem (no skeletal discrepancy)
If etiology is crowding, usually one or two central incisors are involved. This can be treated easily and quickly.
2. Skeletal discrepancy
This is when more than two central incisors are involved, Skeletal component exists. Mandible is positioned forward than maxilla.
Can jaw protruding habit worsen anterior crossbite?
No. Mandible doesn’t grow more when mandible is forced to move forward. Not even for 24 hours a day. Researches showed that fixed mandibular advancement appliances such as Herbst appliance did not grow mandible,
And jaw habit lasts for only a few hours. It doesn’t affect mandibular growth. Therefore, You can advise the parent not to worry about.
How to diagnose anterior crossbite
Anterior crossbite can be easily diagnosed. Let patients bite down all the way. If lower anterior tooth or teeth are in front of upper, it is anterior crossbite. Layperson can tell.
Differential diagnosis of anterior crossbite
Occlusion at CR will determine difficulty of the treatment. Why should we take CR record? Because CR is the starting point of tooth movement.
If edge-edge bite is found at CR, it usually can be corrected in 3-6 months. But if dental compensation exist, it gets more difficult.


How to assess treatment difficulty
1. Functional (pseudo) vs skeletal Class III malocclusion
What is functional Class III malocclusion?
Functional Class III malocclusion refers to Cl III malocclusion where mandible shifts from edge-edge at CR to anterior crossbite at CO. It is found when skeletal discrepancy is not too severe.
Treatment time varies among functional Class III malocclusion. If posterior open bite is severe at CR, treatment takes longer. In the picture below, huge posterior open bite is observed at CR. For this patient, it took over a year to reduce posterior open bite in the lower row of the picture. Still, you can see posterior open bite, but at that moment, functional shift was eliminated and patient doesn’t have anterior crossbite. ,

On the contrary, if there is no premature contact when patient is closing the mouth (if there is no functional shift between CR and CO records), anterior crossbite condition is more severe. The prognosis of the anterior crossbite can be guarded. In this case, dentist or orthodontist may consider deferring treatment for anterior crossbite later because treatment outcome may not be favorable or possible.
2. Torque of the upper and lower incisors (dental compensation)
If upper incisors are already labially flared and lower incisors are lingually inclined, it means anterior teeth have compensated to accommodate skeletal discrepancy. The case has more skeletal problem than the amount of negative overrjet it shows. If bucco-lingual axises of upper and lower anterior teeth were normal, anterior crossbite would have been worse (more negative overjet).
What is dental compensation?
In the picture below, upper anteriors are already flared forward. In this way, anterior crossbite doesn’t look too bad. Horizontal overlap (overjet) looks less tha 1 nn.. The patient’s upper anterior teeth have compensated for sagittal jaw discrepancy by adjusting axial inclination of anteriors. This is called “Dental compensation”
Difficult case- upper incisors are already labially flared

Anterior crossbite in primary dentition
When is good time to treat anterior crossbite
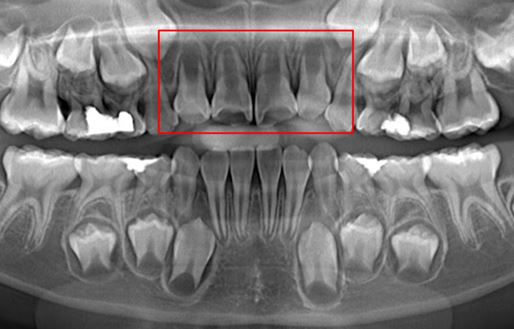
Usually, treatment timing of anterior crossbite is at mixed dentition. Proffits recommended to correct anterior crossbite at early mixed dentition when anteriors have erupted. In my private office, I observe root formation of upper incisors. I like to start treatment when roots of upper incisors are sufficient. Safe time will be when more than 2/3 of roots are formed on central and lateral incisors.
In the picture below, roots of upper 4 incisors are still premature. I defer treatment in this situation unless.
Why it is better to correct anterior crossbite in mixed dentition?
1. Eruption axis of permanent anterior teeth are more buccally inclined that that of primary teeth, So we hope the anterior crossbite improves when new teeth erupt
2. Molars are not available for banded palatal expander (When banded headgear is used)
3. Cooperation of the child may not be good .
Can we treat anterior crossbite in primary dentition?
Yes, why not? Anterior crossbite can be corrected in primary dentition if the child cooperate nicely and permanent incisors are expected to erupt in a year or later..
Advantages of treating anterior crossbite in primary dentition
- Faster treatment time
- Prevention of disturbance in maxillary development in earlier agel
- Less attrition of upper incisors
- Relief of parent’s concern
Teeth moves even faster in younger children. Because I can use horseshoe appliance instead of facemask, palatal expander is not needed. Therefore unerupted maxillary first molars is not a problem.
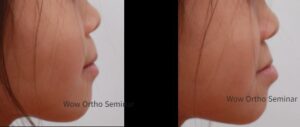
Pictures in the below were my hygienist’s 5-year-old daughter. Mom’s concern was protruding mandible when eating and bruxism. Horseshoe appliance was delivered and anterior crossbite was corrected in 2 months.

/Anterior crossbite was treated in primary dentiton
Facial profile was improved after the treatment.
How to correct anterior crossbite
Treatment of single tooth anterior crossbite

Anterior crossbite of upper lateral incisor
Before starting treatment, comprehensive evaluation is required. It includes lateral cephalometric analysis, panoramic X-ray, photographs, and clinical examination, If only one tooth is in crossbite, it is usually because of the crowding. Dental crossbite involves localized tipping of a tooth or teeth and does not involve basal bone(1). In the simple anterior dental crossbite, the patient displays a normal skeletal pattern and affected incisors present abnormal axial inclination (3).
Root development
Treatment of Anterior crossbite with multiple teeth
Traditionally, anterior crossbite has been treated with facemask. Daily wearing time is 12 to 14 hours. Positive overjet can be achieved usually in 3 to 6 months. In mild case, it can be corrected within a month. Two extraoral elastics with 8 oz force is used.
Most of the time, expander is placed in the upper. If expansion of upper is not needed, Proffit stated that the expander is not needed.


Treatment options for anterior crossbite
This will be a great news. Facemask has been a golden standard for treating anterior crossbite in young children. I learned to use facemask when I was a orthodontic resident at St.
I stopped using facemask in 2020. Instead, I use horseshoe appliance. It is much easier for patient and for me.
-Dr. Kim
Disadvantage of facemask in anterior crossbite treatment
Unfortunately, facemask therapy has side effects such as downward and backward rotation of the mandible This means you can make your patient’s face longer! For this reason, facemask therapy is not recommended to patients with long face. Horse shoe appliance has less tendency of downward and backward rotation of the mandible. Most of all, patients and Mom are relived to find out that they don’t have to use facemask.
Some parents research internet to find out alternative treatment option for facemask.
Horseshoe appliance for treating anterior crossbite
In contrast, horseshoe appliance has less tendency to rotate mandible downward and backward. This appliance may be new to you. I learned horseshoe appliance form Dr. Sung Hun Kim and Dr. Kyu Rim Chung, who invented Biocreative therapy.

Yes. Horseshoe appliance is not orthopedic appliance. It is intraoral appliance. But how much orthopedic effect do you get from facemask? Does facemask induce growth of maxilla? Or does it prevent excessive mandibular growth? Not really.
“The amounts of orthopedic effect is minimal with facemask or headgear”
-Dr.Kim
How does it correct anterior crossbite?

You can see there is functional shift. When the patient bites down, there is premature contact on central incisors. Then, mandible is forced to move forward to achieve maximum intercuspation. Do you remember what type of Class III malocclusion this is? Yes, it is functional Class III malocclusion.
When anterior crossbite is corrected, the patient will have profile like upper left picture.
How long does it take to correct anterior crossbite?
You may wonder the treatment time. Correction of single tooth crossbite can take a month or two.
Treatment time of anterior crossbite of multiple anterior teeth depends on the amount of posterior open bite at CR. Even when anterior crossbite is corrected at centric relation (CR), patient will tend to protrude their jaw when eating if upper and lower posteriors are far away.

Management of relapse of anterior crossbite
Anterior crossbite can relapse again in 6 months or 1 year ever after achieving good overjet.
- Expect recurrence of anterior crossbite
- Educate parent about possible relapse- Patient’s parent may perceive that once their child get phase I treatment for anterior crossbite, it will never occur again. Make them understand that tendency for mandible or lower incisors to move forward is determined in the gene. If patient’s gene has strong mandibular tendency, it cannot be prevented with orthodontic treatment. If patient has skeletal Class III malocclusion and there is no functional shift, the condition may be severe. That’s why we may defer treatment at all.
- Use horseshoe appliance as a retainer and advise patient to wear them at night.
Conclusions
- Anterior crossbite in child needs to be corrected early because maxillary development can be inhibited if anterior crossbite is maintained for long time. Ideal time for the treatment is when 3/4 of roots of upper anteriors are formed.
- Anterior crossbite of single tooth is mostly due to dental problems. In this case, it can be fixed simply with removable appliances or partial bonding of fixed appliances. For anterior crossbite with functional shift, facemask has been the standard treatment of choice. For patients with long face, horseshoe appliance is better choice because it does not have downward and backward rotation of mandible.
- It should be noted that anterior crossbite tendency can reoccur even when ideal overjet was achieved. Clinicians should be aware of this and parent education is critical.
References
- Bayrak, Sule, and Emine Sen Tunc. “Treatment of anterior dental crossbite using bonded resin-composite slopes.” European Journal of Dentistry 2.04 (2008): 303-306.
- Bayrak S, Tunc ES. Treatment of anterior dental crossbite using bonded resin-composite slopes: case reports. European Journal of Dentistry. 2008;2:303–307
- Tse CS. Correction of single-tooth anterior crossbite. Journal of Clinical Orthodontics.