
Principle 1. Build blue-print of treatment outcome with virtual tooth setup for every patient

Let’s stop doing reactive orthodontics. Instead, perform proactive orthodontics. This may be usual orthodontic diagnosis and treatment planning.
Diagnosis:
Skeletal Class II malocclusion (normal maxillary position, Slightly retruded mandible)
Dental Class II malocclusion with deep bite
Moderate crowding in the lower
Treatment plan
Non-extraction, Resolve crowding with interproximal reduction (IPR)
We diagnosed the patient’s condition but the treatment plan usually is just “Non-extraction”. If it is a simple case, it will be fine. But in many cases, We start treatment without assessing the final tooth position. We just bond brackets and place archwire and see how teeth move. A month later, we observe how teeth have moved and react to new tooth position.
Now it’s time to do proactive orthodontics. It may be similar to the treatment planning sequence of Invisalign. We don’t make Invisalign trays after observing tooth movement at each appointment. We plan ahead and make complete sets of the Invisalign trays in advance.
Principle 2. Use light force whenever possible
What are benefits of using light force?
- Patient discomfort will reduced significanly. Many of your patients will say “I didn’t have any pain.”
- Teeth move faster
Quiz 1) What would you do if your patient slight or minimum pressure without any pain when you placed archwire or powerchain?
1) Replace with bigger archwire until patient feels alight discomfort or pain
2) Leave as it.
Quiz 2) Patient calls your office and says, “What should I do if I can’t sleep after tightening my braces?”
The reason for toothache right after tightening braces is the archwire was too big or stiff for the current tooth alignment.
Assistant: What archwire do you want me to put?
Dr.Alexander Put the thickest archwire you can place.
In the past, we tried to squeeze bigger archwire into the bracket slot or we cooled down the NiTi wire with dry Ice so that we can put thick wire. But this is against biology.
Principle 3. Target tooth approach will reduce treatment time and adverse reactions, and improve patient discomfort,
This is especially important for adults patients. Examples
Principle 4. Adopt sagittal- first philosophy to maximize treatment efficiency and patient motivation
Quiz. How would you correct Cl II relationship and level upper anteriors in 4 months? To watch mini-lecture videos, please fill-out your email below.
Principle 5. Take clinical photos every appointment and evaluate progress
I was famous among faculties and residents for taking progress pictures every time when patients come when I was an orthodontic resident at St.Louis University. Why I did it? Because I was looking forward to becoming an orthodontist. That was my dream since I was a 2nd year dental school student.
I still take clinical pictures every time I see a patient. I learn a lot from progress pictures. Things look the same if you just visually examine but you can tell big change in the clinical pictures.
Principle 6. Use patient’s muscular force in open bite patients
We tend to focus on brackets, archwire, and elastics to move teeth. But patient’s muscle force can do wonder.
Principle 7. Use cone beam CT to fully evaluate patient’s oral condition
Why do we need to take cone beam CT when there is no impacted tooth?
- Evaluation of space for molar distalization

* Bucco-lingual crown torque
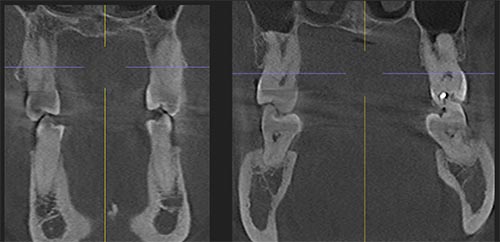
Which side has more stable occlusion? Which side can you expand arch width by buccal tipping movement?
mage by vectorjuice on Freepik